
HAIR TRANSPLANT
Female Hair Transplant
Female hair transplant in Istanbul — no-shave DHI technique for frontal recession, crown thinning, part-line widening and density loss. Full pre-operative medical work-up to identify reversible causes first. Medical oversight Dr. Güleş. All-inclusive package from €2,450.
from €1,780 All-inclusive
Trusted by 10,000+ international patients
JCIAccredited Hospitals
T.C.Ministry of Health Licensed
ISAPSBoard-Certified Surgeons
4.9 ★Trustpilot · 1,200+ reviews
15+ yrsYears of Experience
8,000+Procedures Performed
Global Price Comparison
Save up to 87% in Istanbul
Typical all-inclusive prices by country. Sources: ASPS, RealSelf, major UK/US clinic rate sheets, 2025.
🇹🇷
Turkey (Istanbul)
from €1,780
save 87%
🇬🇧
United Kingdom
from €9,000
🇺🇸
United States
from €13,500
🇮🇹
Italy
from €6,000
🇩🇪
Germany
from €7,000
What's Included
VIP airport transfer (pickup & drop-off)
Accommodation in 4-star partner hotel
Professional translator with 24/7 support
All hospital and surgery fees
Pre-operative blood tests & medical consultation
Anesthesia (general or local as required)
Post-operative medications & aftercare kit
1-year follow-up consultations
Dedicated WhatsApp patient coordinator (24/7)
Not Included
International flights to and from Istanbul
Additional hotel nights beyond the package
Personal expenses (minibar, spa, shopping)
Your Surgical Team
Meet Your Surgeons
Duration
6–8 hours
Anesthesia
Local anesthesia
Hospital Stay
Day procedure
Back to Work
2–3 days
Recovery Time
7–10 days
Results Visible
9–12 months
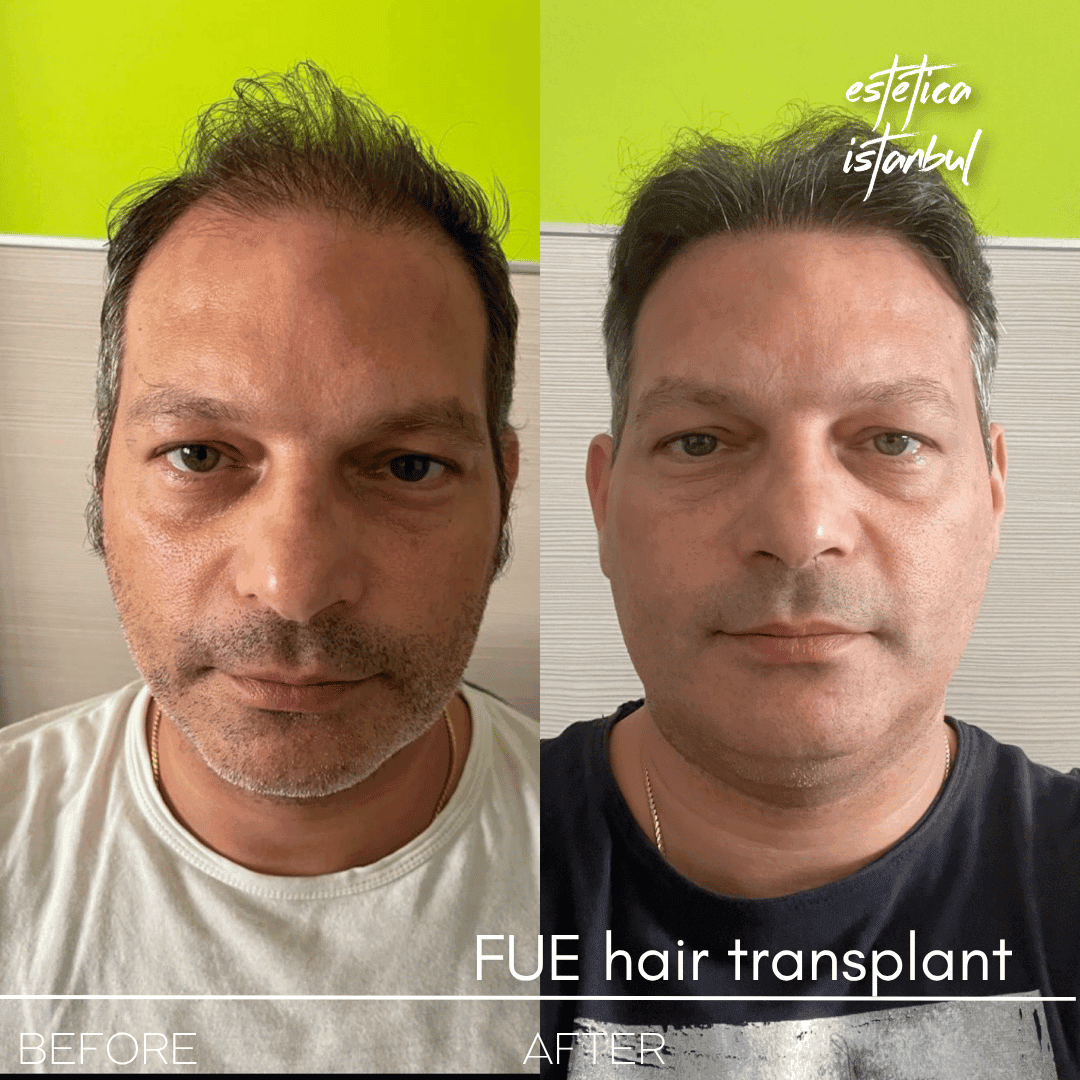
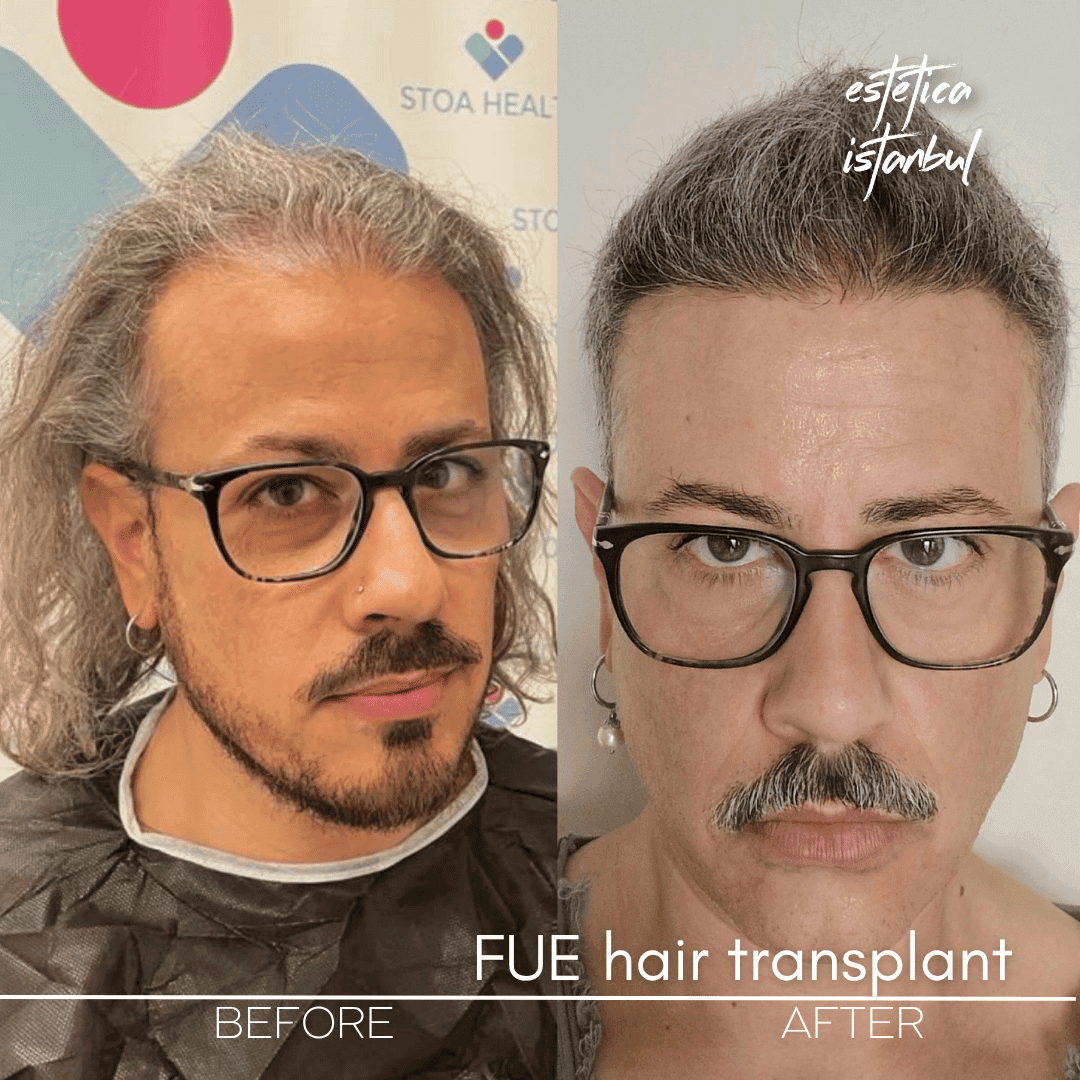
Patient Stories
What Our Patients Say
Frequently Asked Questions
Is hair transplant different for women?
Yes. Female hair loss patterns differ from male pattern baldness. Women typically experience diffuse thinning rather than a receding hairline. Our surgeons use specialised techniques to add density without shaving the entire head — only a small donor strip is trimmed and hidden by existing hair.
Do women need to shave their head for hair transplant?
No. We offer unshaven or partially shaven techniques for female patients. A small area in the donor zone is trimmed short and concealed by your existing hair. You can return to social life without anyone knowing you had a procedure.
How much does female hair transplant cost in Istanbul?
Female hair transplant at Estetica Istanbul starts from EUR 1,950 all-inclusive. The total cost depends on the number of grafts needed. Most female patients require 1,500 to 3,000 grafts to achieve meaningful density improvement.
What causes hair loss in women?
Common causes include hormonal changes (menopause, thyroid conditions, post-pregnancy), genetics, stress, nutritional deficiencies, and traction alopecia from tight hairstyles. Our surgeon will evaluate your cause during consultation to ensure transplant is the right solution.
When will I see results after female hair transplant?
The timeline is the same as male transplants. Transplanted hairs shed at 2 to 4 weeks, new growth begins at 3 to 4 months, and full results are visible at 12 to 18 months. The transplanted hair is permanent.
Get Your Free Consultation
Our medical team will review your case and send you a personalized treatment plan within 24 hours.
Female hair transplant is the most diagnostically complex procedure in the hair-restoration category. The reason: between 40 and 60 per cent of women presenting with hair loss have a treatable underlying medical cause — thyroid dysfunction, iron deficiency, polycystic ovary syndrome, post-partum telogen effluvium, chronic stress, medication side-effects. Transplanting on top of an ongoing medical process produces a poor result: the transplanted hairs will survive, but the native hairs around them will continue to thin, and the overall density will appear lower at six months than before surgery.
For this reason, every female patient we see begins with a pre-operative medical work-up. Blood work (thyroid function, iron panel, vitamin D, B12, folate, hormonal profile where indicated), scalp trichoscopy, and a detailed history are the first steps — not the extraction chair. For a significant proportion of female patients who come to us, the right answer after work-up is not surgery: it is targeted medical treatment that will restore density without any transplantation, at a fraction of the cost. We say so honestly.
Only when the medical causes have been investigated and either ruled out or treated, and when the pattern is a genuine androgenetic or scar-related pattern, do we proceed to surgical planning.
Who female hair transplant is suitable for
The right candidate has completed a medical work-up and either has no reversible cause or has had the reversible cause addressed; has a stable hair-loss pattern (not actively shedding) for at least 12 months; has a pattern suitable for transplantation — female androgenetic alopecia with frontal recession, crown thinning, part-line widening, or with scar-related localised alopecia from traction, surgery, injury or cosmetic procedures; has adequate scalp donor density in the donor zone at the back of the head (female-pattern loss typically spares this zone); is at least 25 years old (younger patients rarely have stabilised patterns); and is a non-smoker at the time of surgery or has stopped four weeks prior.
Who is not a candidate — or not yet: any patient with untreated thyroid dysfunction, unaddressed iron deficiency, untreated PCOS, post-partum telogen effluvium still within its natural 12-month resolution window, or diffuse unpatterned shedding suggestive of an underlying medical cause. We see these patients regularly, and the right answer is medical first, surgical later (if needed at all).
No-shave DHI — the female-specific technique
For female patients, the "no-shave" (or "minimal-shave") DHI technique is preferable to conventional hair transplant for one simple reason: women do not want to return to work with a buzzed head. Conventional FUE requires shaving the donor zone and often the recipient zone entirely, producing a 2–3 week window where the patient's hair is obviously short.
In the no-shave technique, only a small section of the donor zone at the back of the scalp is trimmed — a zone that is covered by surrounding hair and remains invisible once the patient styles normally. The recipient zone is not shaved at all. The grafts are extracted through the surrounding unshaved hair and implanted using DHI Choi pens through the existing native hair. Recovery is dramatically more discreet: women typically return to social and professional life within 5–7 days without anyone noticing.
The technique is slower and more technically demanding than conventional FUE — which is why it is more expensive at serious clinics, and why low-cost clinics often do not offer it. We consider it essential for female patients and we include it in our package.
The medical work-up — what is included
Every female hair transplant starts with the following, before any surgical planning:
Blood work: TSH, free T4, ferritin (iron storage), serum iron, vitamin D, vitamin B12, folate, full blood count, and hormonal profile (DHEA-S, total testosterone, free testosterone, SHBG) when PCOS or androgenic patterns are suspected.
Scalp trichoscopy: magnified examination of the scalp and follicle configuration to assess pattern type (androgenetic vs. scarring vs. diffuse) and active-shedding versus stable presentation.
Detailed history: timing of hair loss, post-partum events, medication changes, stress events, family history, prior treatments (minoxidil, finasteride where prescribed off-label for women, PRP, microneedling).
Based on the work-up, we recommend either (a) medical treatment first, reassessment at 6 months, surgery only if medical treatment has not produced adequate improvement; (b) combined medical + surgical approach, where minoxidil or other treatment continues through and after surgery; or (c) direct surgical approach if no reversible cause is identified and the pattern is clearly stable.
The session, step by step
Local anaesthesia. Duration six to nine hours depending on graft count (typically 1,500–3,500 grafts for a female patient, reflecting smaller zones than male-pattern work but requiring similar technical precision). Single session for most patients.
The zone at the back of the donor scalp is trimmed (an area roughly the size of a palm, hidden under overlying hair). Grafts are extracted with a 0.7–0.8 mm micro-punch. Grafts are sorted; single-hair grafts prioritised for the hairline and part-line (density matters less than naturalness here); multi-hair grafts placed in the main density zones. Implantation is via Choi implanter pens into the unshaved recipient zone, at the correct angles for each sub-region (part-line, crown, frontal hairline).
Recovery
Week 1
Small crusts on each implantation site, resolving over seven to ten days. Mild redness in the recipient zone. The trimmed donor zone is covered by surrounding hair. Hair can be washed gently from day three using the specific protocol provided. Most female patients return to work between day five and seven, with the existing hair arrangement hiding any remaining signs.
Weeks 2–8
Shock loss of transplanted hairs at week three to four (expected and temporary). Possible mild shock loss of adjacent native hairs (usually recovers). Hair appears thinner during this phase than on the day after surgery.
Months 3–6
New growth begins from transplanted follicles. Density builds progressively.
Months 9–12
Final density and growth characteristics stabilise by month 9–12.
Risks and realistic expectations
Honest risks: folliculitis; shock loss of adjacent native hairs; imperfect angle on a small proportion of grafts; slight donor-zone density reduction that an experienced technique minimises; graft survival below expectation if post-operative instructions are not followed.
Specific risks in female transplant that differ from male: because the underlying medical cause is a bigger factor in female loss, the most important "risk" is operating on a patient whose underlying condition has not been identified and addressed. The transplant will survive, but the non-transplanted native hairs will continue to thin, producing disappointment at one year. This is why our medical work-up is non-negotiable.
Why Istanbul versus other destinations
Turkey's hair-restoration volume is the highest in the world. Our partner clinic combines this volume expertise with a specific female-focused pathway: mandatory pre-operative medical work-up, no-shave DHI technique, female-specific pattern planning, and English-speaking support through the 12-month growth window.
**Dr. Mustafa Ekrem Güleş** provides medical oversight.
Why not the €1,500 female hair transplant
On female transplant, the rock-bottom price is paid most often in the omitted medical work-up — transplanting on top of untreated thyroid dysfunction, iron deficiency or PCOS. The hairs grow; the surrounding native hairs continue to thin; the patient is disappointed at 12 months; and no "revision" surgery will fix the underlying medical issue. Also commonly: full-shave technique applied to a female patient (unacceptable for most women's professional and social lives), and no post-operative support for the anxious months 3–6 when shedding is prominent.
What you pay for with us is verifiable: comprehensive pre-operative medical work-up (blood panel + trichoscopy + history), no-shave DHI technique, female-specific pattern planning, JCI-partnered medical oversight, English-speaking follow-up at 3, 6 and 12 months with specific female-cohort guidance (post-partum considerations, menopause, medication interactions).
English-speaking team — for the full 12-month journey
Our team replies in English on WhatsApp, phone and email. Female hair restoration has specific anxiety windows (the shock-loss phase at months 1–3, the slow early regrowth at months 3–6) that benefit from proactive English-language support. We provide it throughout.
Request your free consultation — our team replies in UK/IE business hours and in a second window covering US Eastern through Australian morning. Photo-based pre-assessment, medical-work-up recommendation, and candidacy evaluation on the same day.
Deep Dive
All articles →Further Reading
Hair Transplant
Scarless Hair Transplant Turkey
Hair transplantation is an important milestone in the journey of individuals to cope with hair loss. Today, with the innovations brought by technology, hair transplantation methods are constantly evolving. One of the most remarkable results of this...
Hair Transplant
Using Shampoo After Hair Transplant
You may have many questions about shampooing, showering and care after hair transplantation. In this article, we have explained how you should wash your hair after hair transplantation. We wish you a pleasant reading. ...
Hair Transplant
First Haircut After Hair Transplant: The Ultimate Guide
When your hair grows after hair transplantation, you may wonder questions such as how should the haircut be, when should it be or how should I style my hair? In this blog post, we have answered these questions in detail. We wish you a...